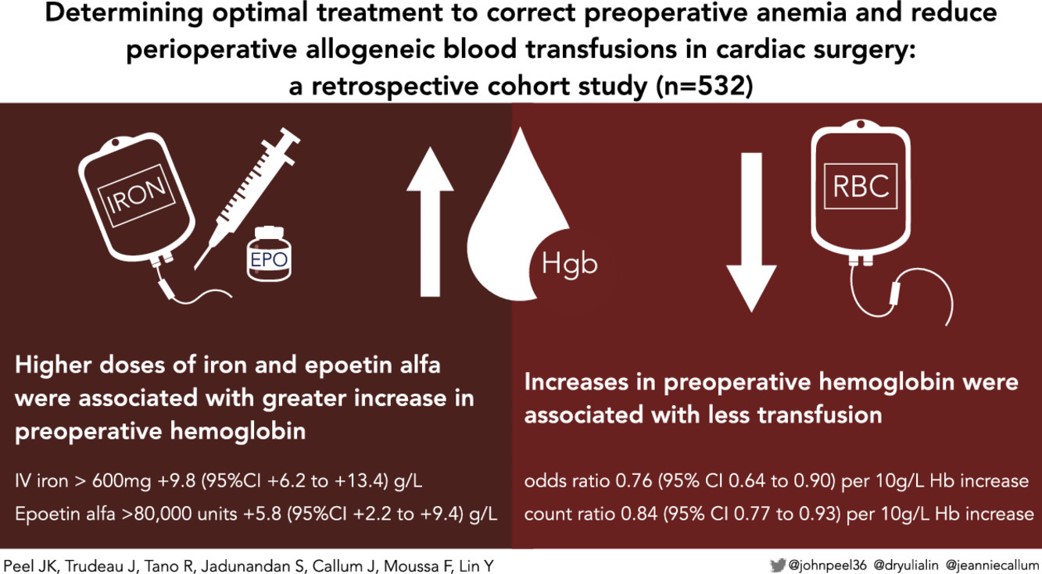
Determining Optimal Treatment to Correct Preoperative Anemia and Reduce Perioperative Allogeneic Blood Transfusions in Cardiac Surgery: A Retrospective Cohort Study
URL: https://www.jcvaonline.com/article/S1053-0770(20)31391-4/fulltext
DOI: https://doi.org/10.1053/j.jvca.2020.12.044
Published: Journal of Cardiothoracic and Vascular Anesthesia
Authors: J.K. Peel, J. Trudeau, R. Tano, S. Jadunandan, J. Callum, F. Moussa, Y. Lin
Click here to read the article for free, thanks to an agreement among EACTA and Elsevier
Article description
- The preoperative anaemia can be associated with a higher risk of transfusion, postoperative complications, more extended intensive care unit and hospital length of stay, and mortality
- Additionally, the red blood cell (RBC) transfusion is associated with increased risk of postoperative morbidity and mortality.
- Patient blood management (PBM), an evidence-based, multidisciplinary approach, is based on the preoperative treatment of anaemia, restrictive transfusion thresholds, and minimizing intraoperative blood loss.
- The need for a transfusion increased when the preoperative haemoglobin (Hgb) level is low. The iron supplementation and erythropoietin are frequently used to correct preoperative anaemia.
- The study aimed to determine the optimal strategy for the treatment of preoperative anaemia using oral iron, intravenous iron, and / or epoetin alfa (Recombinant human erythropoietin) before cardiac surgery. Speci?cally, the authors sought to determine which dose ranges were associated with improved preoperative Hgb and reduced the need for blood transfusion.
Summary:
- A retrospective cohort study included 532 consecutive patients undergoing nonurgent cardiac surgery (CABG, valve, or combined CABG and valve) with or without cardiopulmonary bypass (CPB) from 2008 until 2018.
- Patients received epoetin alfa and / or iron supplementation according to the ONTraC algorithm and followed-up through the perioperative period (https://www.ontracprogram.com/ckupload/files/103/Revised%20PBM%20algorithm%20%202016(1).pdf). The study interventions included treatment with oral iron; therapy with intravenous iron at commonly prescribed dose ranges (?300 mg, 301-600 mg, >600 mg); and treatment with epoetin alfa at commonly prescribed dose ranges (?40,000 U, 40,001-80,000 U, >80,000 U).
- The Hgb concentration was recorded at referral (time of referral), preoperative (within seven days before surgery), nadir (lowest Hgb recorded during admission), and discharge (last Hgb before discharge).
- Using different regression methods, the authors included some potential confounders including the preoperative Hgb, the change from referral to preoperative Hb, the odds of transfusion, the number of RBCs units transfused, and the various treatment options.
- The covariates differ according to the used regression model; they included recipient age, sex, referral or preoperative Hgb, oral iron treatment, intravenous iron, epoetin alpha, duration of therapy, year of surgery, and type of surgical procedure.
- In the entire cohort, mean referral Hgb was 122 (±17) g/L, 374 (70%) patients were referred with Hgb <130 g/L and 123 (23%) patients had iron de?ciency anaemia.
- Patients received either no treatment (111 [16%]), oral iron alone (244 [35%]), intravenous iron (121 [17%]), epoetin alfa (99 [14%]), or combination therapy of intravenous iron with epoetin alfa (117 [17%]).
- Patients treated with intravenous iron and epoetin alfa had, on average, 25 (±28) days and16 (±45) days, respectively from their last dose to the date of surgery. No signi?cant difference was observed across dose ranges of both medicines.
- The multivariate linear regression showed that the more significant changes in Hgb from referral to preoperative value was associated with the treatment with intravenous iron >600 mg (p < 0.0001), treatment with epoetin alfa >80,000 U (p = 0.0017), and referral Hgb (p < 0.0001)
- Higher preoperative Hgb (odds ratio 0.76 [0.64-0.90]; count ratio 0.84 [0.77-0.93] per 10 g/L) corresponded to a lower need for RBC transfusion.
- The Poisson model showed that more RBC units were significantly transfused during CABG plus valve procedures than CABG (CR 2.09 [95% CI 1.41-3.09]; p = 0.0002).
- The main limitations of the present study include (1) retrospective design, (2) non-randomized treatment decision, (3) missing some confounding factors from multivariate analysis (e.g., renal failure, use of CPB, estimated blood loss), (4) minor changes included in the ONTraC algorithm during the study period, and (5) significant missing data.
Conclusions:
- The authors recommend that cumulative preoperative doses of intravenous iron >600 mg and epoetin alfa >80,000 U be used to treat anaemia before cardiac surgery.
Journal of Cardiothoracic and Vascular Anesthesia DOI: (10.1053/j.jvca.2020.12.044)
Copyright © 2021 Elsevier Inc.