Perioperative Serum Free Hemoglobin and Haptoglobin Levels in Valvular and Aortic Surgery with Cardiopulmonary Bypass: Their Associations with Postoperative Kidney Injury
URL: https://www.jcvaonline.com/article/S1053-0770(21)00355-4/fulltext
DOI: https://doi.org/10.1053/j.jvca.2021.04.029
Published: Journal of Cardiothoracic and Vascular Anesthesia (April 26, 2021)
Authors: Mai Hokka, Moritoki Egi, Kenta Kubota, Satoshi Mizobuchi
Article description
- Acute kidney injury (AKI) is a common complication after cardiac surgery with cardiopulmonary bypass (CPB) that is associated with a high rate of postoperative mortality and prolonged hospital and intensive care unit stays.
- Caution should be exercised on the prevention and management of modifiable risk factors.
- Hemolysis frequently occurs in patients undergoing cardiac surgery with CPB because of CPB itself, blood transfusion, and the use of a cell salvage system.
- Hemolysis leads to an increase in serum-free hemoglobin (fHb), contributing to AKI due to microcirculation dysfunction.
- Thus, administration of an fHb scavenger such as external haptoglobin might effectively prevent AKI after cardiac surgery using CPB. It is necessary to consider the followings to explore the efficacy of haptoglobin for preventing AKI:
- The time trends of serum fHb and haptoglobin levels during the perioperative period.
- Their associations with the risk of AKI.
- The value of fHb as an indicator of treatment timing.
- This prospective observational study was designed to (1) obtain the time trends of perioperative fHb and haptoglobin levels and (2) assess the independent associations of fHb and haptoglobin levels with incidence risk of AKI.
- The investigators hypothesized that the perioperative serum-free hemoglobin and haptoglobin concentrations are not different in patients with and without postoperative AKI.
Summary:
- Seventy-four patients who underwent valvular and aortic surgery using CPB were included in this study; 25 (33.8%) of them experienced postoperative AKI.
- Patients with AKI were significantly older (p=0.01) and had a lower preoperative eGFR (p=0.04) than patients without AKI. However, the median value of MAP during CPB in patients was comparable in patients with and without AKI (p=0.49).
- After induction of anesthesia, the median fHb levels were similar in patients with and without AKI (p=0.65).
- The median fHb level increased after the initiation of CPB and reached a peak value of 0.08 (0.06-0.12) g/dL at 30 minutes after weaning from CPB. Compared with patients without AKI, the fHb levels were significantly higher in patients with AKI during and after CPB (p < 0.011).
- Then median fHb level returned to the baseline level on POD 1 with the disappearance of the statistically significant difference (p=0.62).
- The median maxfHb level in patients with AKI was 0.13 (0.12-0.15) g/dL, which was significantly higher than that of 0.08 (0.06-0.11) g/dL in patients without AKI (p<0.001).
- The area under ROC curve >0.7 at maxfHb showed an estimated cutoff value of 0.12g/dL.
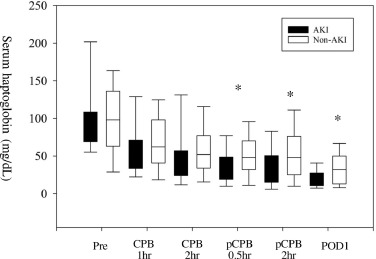
- The haptoglobin levels in patients with AKI were significantly lower than those in patients without AKI from 0.5 hours after CPB until the POD 1 (p<0.041).
- Multivariate analysis for the risk of postoperative AKI demonstrated that maxfHb and minimum serum haptoglobin level during the study period (minHp) were independently associated with increased risk of AKI (maxfHb: adjusted odds ratio=1.33 (95% CI: 1.12, 1.58), p=0.001, minHp: adjusted odds ratio= 0.95 (95% CI: 0.91, 1.00), p=0.03). Additionally, the fHb level had begun to have an independent association with AKI at one hour after CPB initiation.
- However, this study was a small, single-center study conducted in Japan over a six-year period where their results cannot be generalized. Other limitations to the present study included excluding patients with preoperative chronic renal failure and those who received external haptoglobin.