Cerebrospinal Fluid Drainage in Thoracic and Thoracoabdominal Endovascular Aortic Repair: A Survey of Current Clinical Practice in European Medical Centres
URL: https://www.jcvaonline.com/action/showPdf?pii=S1053-0770%2821%2900639-X
DOI: https://doi.org/10.1053/j.jvca.2021.08.003
Published: Journal of Cardiothoracic and Vascular Anesthesia August 6, 2021
Authors: Kavita Houthoff Khemlani, Geert Willem Schurink, Wolfgang Buhre, Jan Uwe Schreiber
Article description
- Spinal cord ischemia (SCI) is a severe complication among 1% to 10% of patients undergoing thoracic endovascular aortic repair (TEVAR) procedures that might result in temporary or permanent neurological insults.
- Several identified predictors for the SCI following TEVAR include the location of the aneurysm, prior distal aortic surgery, perioperative hypotension, emergency procedures, left subclavian artery coverage without revascularisation, and preoperative renal dysfunction.
- Protective measures against the SCI include optimizing spinal cord perfusion using cerebrospinal fluid drainage (CSFD), avoiding systemic hypotension, neuromonitoring for timely intervention, and corticosteroids.
- There is substantial evidence that the preventive use of CSFD might be beneficial in open-repair surgery of thoracoabdominal aneurysms.
- There is no consensus on the indication, timing of placement, and use of CSFD in patients undergoing TEVAR procedures.
- The international guidelines suggest several protection strategies; however, the evidence of these recommendations is usually low.
- The Society for Vascular Surgery recommended prophylactic CSFD for SCI protection in TEVAR patients considered as high-risk cases (level of recommendation: grade 1 [strong], quality of evidence: B [moderate]).
- This survey aimed to evaluate the daily clinical practice in European hospitals regarding the protection against SCI during TEVAR procedures, emphasizing CSFD.
- This survey might help develop other research protocols that lead to high-quality evidence, which is needed to create best practice guidelines for appropriate risk stratification.
Summary:
- An online survey on the current practice of spinal cord protection with an emphasis on CSF drainage was sent to the EACTAIC and European Society of Vascular Surgeons (ESVS) members.
- The response rate was (73.3%) 132 returned responses over 180 invitations were sent. One-hundred-four responses were used for analysis.
- Most respondents (78%) used a written protocol for spinal cord protection during TEVAR in clinical routine.
- The most common protective measures are CSFD (98%), controlled hypertension (73%), pharmacologic agents (14%), and hypothermia (7%).
- Corticosteroids were used by 91% of the respondents as part of a pharmacologic protection strategy, and naloxone was used regularly by only 18% of the respondents.
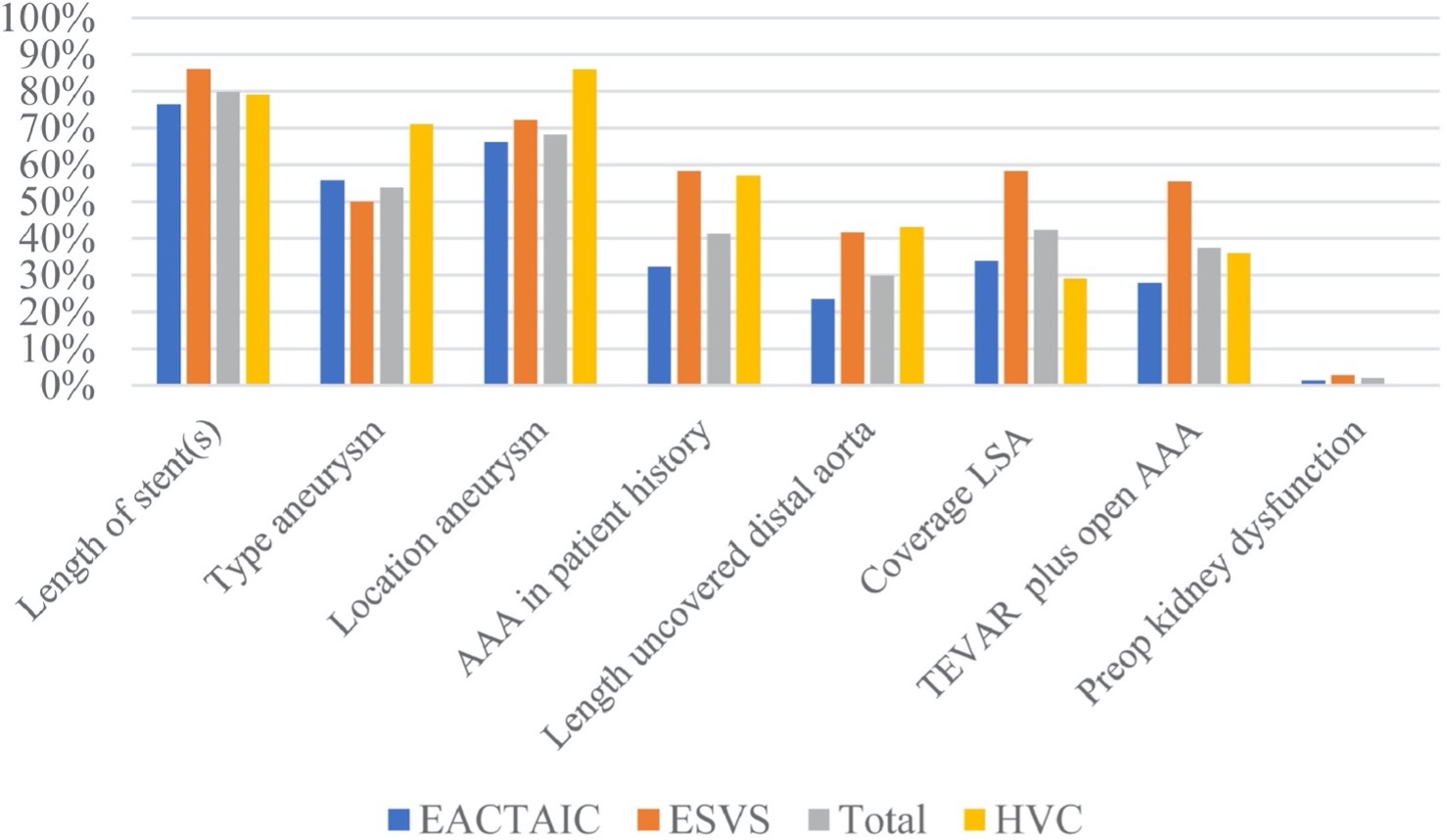
- The two most common indications for placement of a spinal catheter were the length of the stent (80%) and the location of the aneurysm (68%). [Figure 1]
- Most respondents stop vitamin K antagonists, direct-acting anticoagulants, and clopidogrel before placing a CSFD catheter. Aspirin was stopped by only 7% of the respondents.
- Of the included responses in the analysis, 76% preferred placement of the CSFD catheter on the day of surgery. In contrast, 23% of the respondents placed the spinal catheter the day before the procedure.
- Only 40% of the respondents considered CSFD continuous intraoperative CSFD drainage as the most common approach; however, a relevant subset of respondents used other techniques, including drainage as indicated (32%), intermittent drainage (21%), or no drainage (7%). 60% of respondents usually use intraoperative passive drainage, targeting pressures ranging between 8 and 20 cm H2O and the volume targets between 10 and 20 mL/h.
- A total of 13% of respondents from 14 different high-volume centres (HVCs) performed more than 50 procedures annually; of them, five centres performed more than 100 TEVAR procedures per year.
- Eighty-six of the respondents in the HVCs used a predefined written protocol including CSFD and controlled arterial hypertension. CSFD was frequently used based on the length of the stent (79%) and the location of the aneurysm (86%). In general, Crawford type I and II aneurysms indicate placing a spinal catheter in all HVCs.
- A CSFD catheter was inserted as a treatment modality in 57% of HVC respondents compared with 42% of non-HVC respondents.
- The survey has some limitations. First, the survey was limited to EACTAIC and ESVS members, and the given responses and response rate determined the results. Second, the total number of respondents was included for analysis, although some centres yielded more than one specialist. However, this would only have a possible effect on numeric information.
Conclusions:
- There is a variety in the approach regarding indication and timing of spinal catheter placement, management of anticoagulation, and management regarding spinal drain-related complications.
- The authors believe that this overview can aid in the further development of additional high-quality evidence. This is needed to develop best practice guidelines based on appropriate risk stratification.
- This survey identified the contemporary practice regarding CSFD during endovascular aortic repair and quantified areas of consensus and differences.
Figure 1. Indications to place a spinal catheter. AAA, abdominal aortic aneurysm; EACTAIC, European Association of Cardiothoracic Anaesthesiology and Intensive Care; ESVS, European Society of Vascular Surgeons; LSA, left subclavian artery; TEVAR, thoracic endovascular aortic repair.