High versus Normal Blood-Pressure Targets in relation to Right Ventricular Dysfunction after Cardiac Surgery: a Randomized Controlled Trial
URL: https://www.jcvaonline.com/article/S1053-0770(21)00189-0/fulltext
DOI: https://doi.org/10.1053/j.jvca.2021.02.054
Published: Journal of Cardiothoracic and Vascular Anesthesia (March 2021)
Authors: I.T. Bootsma, F. de Lange, T.W.L. Scheeren, J.S. Jainandunsing, E.C. Boerma
Article description
- Right ventricular (RV) dysfunction is an underestimated clinical entity associated with low-cardiac-output syndrome and increased mortality after cardiac surgery.
- Induced increases in blood pressure can improve right coronary artery blood flow, re-establish the transseptal gradient, and right ventricular (RV) and left ventricular dimensions, resulting in improved RV function.
- Thus, the direct inotropic effect of norepinephrine (NE) on the right ventricle might be conceivable.
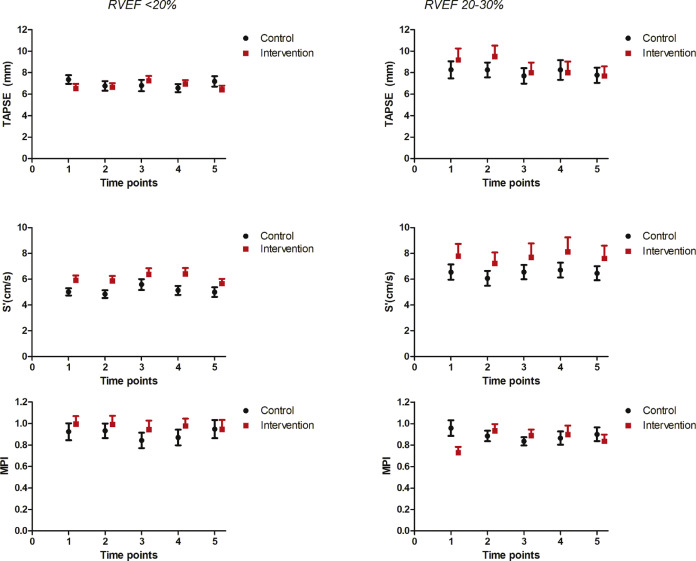
- The investigators studied the norepinephrine-mediated effect of high versus normal blood pressure targets on RV function after cardiac surgery patients with a low (<20%) or moderate (20%-30%) RV ejection fraction (RVEF).
- They hypothesized that higher blood pressure would improve RV function.
Summary:
- The study included 78 patients who had postoperative RVEF <30% in combination with a mean arterial pressure (MAP) of ?65 mmHg within the first postoperative hour in the intensive care unit (ICU) after cardiac surgery through full sternotomy.
- Patients were classified into two groups; (1) a low RVEF (<20%) and (2) moderate RVEF (between 20% and 30%), as measured by the PAC on admission to the ICU.
- Postoperative ventilation was standardized using a respiratory frequency of 20-to-25 times per minute, tidal volumes of 6 mL/kg ideal body weight, and a postoperative end-expiratory pressure of 10 cmH2O.
- In each group, patients were assigned randomly to either a normal-target blood pressure (MAP 65 mmHg) group or a high-target blood pressure (MAP 85 mmHg) group with titrating norepinephrine infusion.
- The primary outcome was the change in RVEF over a one-hour study period.
- In the RVEF<20%, there was no significant between-group difference in the change in RVEF (–1% [–3.3 to 1.8] in the normal-target group v 0.5% [–1 to 4] in the high- target group; p = 0.159).
- Similarly, there was no significant between-group difference in the change in RVEF (–1% [–3 to 0] in the normal-target group v 1% [–1 to 3] in the high-target group; p = 0.074).
- These observations were in line with the documented no improvements in RV echocardiographic parameters (i.e., TAPSE, S’, and myocardial performance index) in the intervention group.
- The study is limited with the limited number of patients and the short window of one-hour observation.