Non-transvenous Cardiovascular Implantable Electronic Device Technology: A Review for the Anesthesiologist
URL: https://www.jcvaonline.com/article/S1053-0770(21)00113-0/fulltext
DOI: https://doi.org/10.1053/j.jvca.2021.02.018
Published: Journal of Cardiothoracic and Vascular Anesthesia (February 10, 2021)
Authors: Joseph Cody, Thomas Graul, Scott Holliday, Scott Streckenbach, Nasir Hussain, Adam A. Dalia, Brett Cronin, Jennifer Hargrave, John G. Augoustides, Michael Essandoh
Article description
- This narrative review addresses the features and capabilities and provides guidance for perioperative management for non-transvenous leadless cardiac implantable electronic devices, such as the Micra and the subcutaneous implantable cardioverter-defibrillator.
Summary:
- Micra Systems
- Three leadless pacing systems are available: the Micra VR, the Micra AV (Medtronic, Minneapolis, MN), and the Nanostim (St. Jude Medical/Abbott Laboratories Chicago, IL).
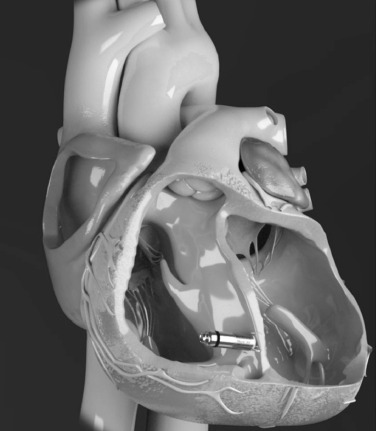
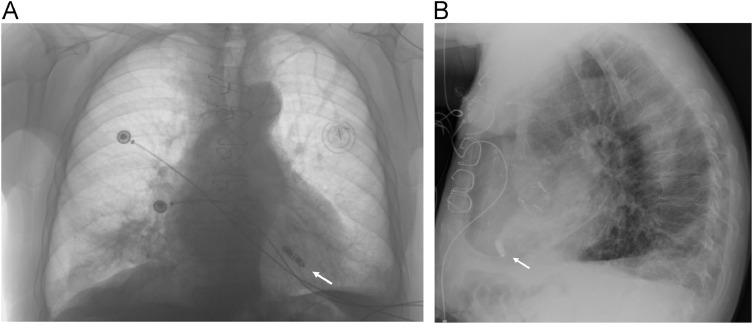
- The Micra leadless transcatheter pacing systems are single chamber miniaturized bipolar pacemakers implanted in the right ventricle (RV) by four nitinol tine through a percutaneous transfemoral venous approach to treat bradyarrhythmias. These include;
- The “Micra VR” provides RV pacing only, with a battery life of approximately 12 years and no support for atrioventricular (AV) synchrony, anti-tachycardia pacing (ATP), or defibrillation therapy. However, standard programmers can program it.
- The “Micra AV” is nearly identical to the Micra VR but with an added feature of AV synchronous pacing, which potentially improves biventricular stroke volumes. Unlike conventional AV synchronous pacing with accurate atrial signal detection with a right atrial lead, it provides RV pacing by detecting mechanical right atrial contractions via an accelerometer. Thus, AV synchronous pacing during thoracic procedures may be ineffective because the Micra may track surgery-related tissue motion and may pace the RV asynchronous to the sinus node. The Micra AV has two automated mode-switching features (activity mode switch and AV conduction mode switch) that can potentially improve hemodynamics and preserve battery life.
- Anesthetic Considerations for Micra Patients
- The anesthesiologist should consider a careful preoperative assessment, including the type of surgery, concern for electromagnetic interferences (EMI), type of Micra, indications for placement, current device settings, and degree of pacing therapy dependence.
- Communications with the primary cardiologist, electrophysiologist, or CIED support team member might be needed to guide perioperative management.
- The magnet application is not an option in Micra leadless pacemakers as they do not possess a magnet response and pacing rates only can be altered by reprogramming the device.
- The decision to reprogram a Micra device depends on the surgery site and concern for EMI during the procedures requiring monopolar electrocautery. For example, if surgery is above the umbilicus, over-sensing from EMI may cause bradycardia and hypotension.
- In addition, reprograming the Micra to an asynchronous mode might be considered for the pacing-dependent patient.
- Suppose reprogramming is not possible in case of emergency procedures. In that case, caution should be exercised to reduce the risk of potential harm from EMI inhibition of pacing, such as vigilant hemodynamic monitoring, the placement of the grounding pad to not pass near the Micra, and avoidance of monopolar electrocautery if possible.
- In general, reprogramming to asynchronous pacing may cause the R-on-T phenomenon and ventricular fibrillation and should be avoided. Instead, it may be best practice to leave the Micra in VVI pacing mode (no reprogramming) and use bipolar electrocautery or brief periods of monopolar electrocautery.
- Placement of intracardiac catheters, such as a Swan-Ganz catheter, may cause pulmonary embolization, especially within a few months of Micra insertion as the tines may be partially endothelialized.
- Additionally, treatment of right ventricular systolic failure with temporary percutaneous mechanical circulatory support devices, such as the Impella RP or a PROTEK Duo, may cause embolization of the Micra into the pulmonary circulation.
-
S-ICD System
- The S-ICD system provides defibrillation treatment of life-threatening ventricular arrhythmias for patients with inadequate vascular access, those at high risk of infection, and not expected to require bradycardia pacing or CRT, with no associated leads-related complications.
- The device can deliver up to five nonprogrammable, 80-joule shocks per ventricular tachycardia or ventricular fibrillation episode. The S-ICD does not offer ATP therapy or sustained bradycardia pacing capabilities aside from 30 seconds of postshock bradycardia demand pacing at 50 pulses-per-minute bradycardia <50 beats per minute.
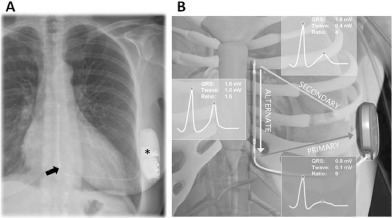
- The ‘S-ICD’ system has a pulse generator implanted subcutaneously or intramuscularly between the serratus anterior and latissimus dorsi muscles along the left midaxillary line. The generator is connected to the single subcutaneous lead, which is tunneled along the left parasternal border.
-
Anesthetic Considerations for S-ICD Patients
- The anesthesiologist should exercise caution to avoid inappropriate S-ICD shock therapies, which can induce ventricular fibrillation and the need for additional shocks.
- Communications with the CIED team or electrophysiologist should be considered to gather information on S-ICD programming (e.g., magnet response, which enables temporary magnet suspension of shocks, and shock therapy) and other information on battery longevity and lead impedance.
- A transcutaneous defibrillator with the placement of the defibrillation pad placement far away from the pulse generator should be available to treat life-threatening ventricular arrhythmias.
- In light of having a larger sensing area, the EMI can cause inappropriate S-ICD shock therapies and also may inhibit postshock bradycardia pacing by the device.
- S-ICD shocks can be suspended with a magnet placement over the pulse-generator header or lower aspect or programmed off. Correct placement of the magnet is confirmed with hearing beeping tones (r-wave synchronous) within one second and will end after 60 seconds.
-
Non–TV-CIED Innovations Under Investigation
- Several innovative technologies will soon become relevant to perioperative anesthesia patient care, including a wireless endocardial left ventricular (LV) leadless pacing system and a modular pacing and S-ICD system.